She’s the busty new girlfriend of Tammy Hembrow’s ex-fiancé, Reece Hawkins.
And London Goheen, 20, has admitted to having breast implants.
The brunette bombshell made the revelation to Instagram on Monday.
‘Where did you get your breasts done?’: Reece Hawkins’ girlfriend London Goheen admits to having a boob job. Pictured left in 2016 and right in 2017
‘Where did you get your breast augmentation you look amazing,’ one fan asked to which London replied ‘Houston.’
A boob job is not the only thing the American beauty is believed to have had done.
Speaking to Daily Mail Australia last month, plastic surgeon Dr Randal Haworthclaimed the Texan had undergone rhinoplasty and non-surgical lip fillers.
Candid: ‘Where did you get your breast augmentation you look amazing,’ one fan asked to which London replied ‘Houston’
Busty: London is known for her Barbie doll-like proportions
‘It is clear to me her previously pleasing nose has been further refined with rhinoplasty,’ said Dr Haworth.
‘Specifically, her slightly bulbous tip has been narrowed to form a perfect streamline with her thin nasal bridge. All-in-all, it’s good work.’
Dr. Haworth further speculated that London has augmented her lips with filler to create a more ‘sensual’ look.
‘Her lips have been obviously augmented, most likely with a hyaluronic acid filler such as Juvéderm, Volbella or Restylane,’ he said.
Expert opinion: ‘It is clear to me her previously pleasing nose has been further refined with rhinoplasty,’ a surgeon said of London. Pictured left: in her teenage years, and right: in 2018
London first made headlines in September when Reece Hawkins publicly confirmed they were dating.
The new relationship began just months after Reece ended his engagement to fitness model Tammy Hembrow, leaving fans devastated.
Reece and Tammy – who share two children, Saskia and Wolf – rose to stardom on social media back in 2014.
Many fans weren’t happy to see the District Goods designer move on so quickly, with London herself targetted by trolls.
Ex files: London is now dating Reece Hawkins, who is the ex of social media star Tammy Hembrow (both pictured)
She is one of Australia’s most glamorous women, but has Kyly Clarke (née Boldy) had a little help achieving her flawless appearance?
According to Beverly Hills plastic surgeon Dr Randal Haworth, the cricket WAG, 37, has seemingly undergone subtle changes over the years.
Speaking exclusively to Daily Mail Australia, Dr Haworth claimed that Kyly appears to have invested in non-surgical lip fillers.
EXCLUSIVE: ‘Her features are sublime’: A Beverly Hills cosmetic surgeon has claimed Kyly Clarke may have had a little help achieving her flawless appearance. Pictured left: in an old Captain Snooze commercial, and right: in a recent Instagram photo
‘Kyly, needless to say, is a very attractive young woman, and the envy of both men and women alike,’ Dr Haworth began.
‘Her features are sublime with a defined jawline, classic cheekbones and the most alluring of feline eyes.’
He observed: ‘Certain photographs of Kyly suggest she may have had her lips plumped with a filler of sort, most likely a hyaluronic acid such as Juvéderm.’
Plump pout: Speaking exclusively to Daily Mail Australia, Dr Randal Haworth claimed that Kyly appears to have undergone non-surgical lip fillers. Pictured in a recent Instagram photo
Changes: Dr Haworth observed, ‘Certain photographs of Kyly suggest she may have had her lips plumped with a filler of sort, most likely a hyaluronic acid such as Juvéderm’. Pictured left: in a KFC commercial from circa 2010, and right: in a recent Instagram photo
‘Hopefully this is just lighting and lip gloss because Kyly’s lips need no help in the beauty department!’ he added.
Last year, another cosmetic expert, Dr Meaghan Heckenberg, told Woman’s Day she ‘suspect[ed] Kyly had some jaw slimming with Botox’.
Kyly has never admitted to having plastic surgery, but she told Daily Mail Australia in an April 2016 interview that she was open to the idea.
Refined features: Last year, another cosmetic expert, Dr Meaghan Heckenberg, told Woman’s Day she ‘suspect[ed] Kyly had some jaw slimming with Botox’. Pictured recently on Instagram
‘I think at the end of the day, each to their own. I don’t knock anyone for doing whatever they choose to do. If that’s what you want to do with your life, that’s okay,’ she said at the time.
She added that her Maltese heritage was the secret behind her ageless complexion: ‘I am lucky with my skin. My mum is Maltese and she has really really good skin.’
Kyly, who is a former model, has been married to retired cricketer Michael Clarke, 37, since 2012.
Never say never! Kyly has never admitted to having plastic surgery, but she told Daily Mail Australia in an April 2016 interview that she was open to the idea
According to Dr Haworth, 47-year-old fitness guru Michelle Bridges may have undergone a transformation in recent years thanks to cosmetic enhancements.
‘It appears Michelle’s striking facial change came from an enthusiastic use of fillers and Botox,’ he told Daily Mail Australia
‘I have a small suspicion Botox was also injected in and around her chin because her smile in recent pictures seems somewhat restricted and stiff.’
While Michelle is yet to confirm whether she has indulged in these treatments, she has previously supported the use of non-surgical enhancements.
In 2014, she said of cosmetic work such as Botox: ‘I am a fan of anything that makes a person feel good about themselves and more confident.’
After inspecting recent photographs of Elle Macpherson, Dr Haworth believes that she may have had a subtle rhinoplasty in her thirties, resulting in ‘a squared nasal tip flanked by vertical grooves extending down to her nostril rims’.
He also claims that she may have gone under the needle to enhance her already-striking visage.
However, Elle has long been an advocate of natural beauty, crediting an active lifestyle and a plant-based diet as the secrets behind her age-defying appearance
She told This Morning in June: ‘I haven’t done any plastic surgery, not that I have any judgement – it just hasn’t been my choice. I like a natural looking face.’
But in 2016, Elle admitted to People magazine that she had experimented with cosmetic procedures to fight wrinkles.
‘Of course I think about lines. There have been times in my life when I have tried really hard to get rid of them [such as with fillers], and it doesn’t work. So I tend to leave all that alone as much as possible,’ she said.
Observations: After inspecting recent photographs of Elle Macpherson, Dr Haworth believes she may have had a subtle rhinoplasty in her thirties, resulting in ‘a squared nasal tip flanked by vertical grooves extending down to her nostril rims’. Left: Elle in 2002, and right: in 2018
Dr Haworth claims Home and Away star Ada Nicodemou, 41, has stayed ‘on point’ in her career thanks to ‘various non-surgical cosmetic treatments’.
However, he also believes the mother-of-one has undergone a breast augmentation, in addition to using fillers and Botox.
While Ada is yet to reveal whether she has gone under the needle, she has previously supported the use of enhancements in an interview with Daily Mail Australia.
‘I just think everyone should do whatever makes them feel good… I have no judgement on [Botox] whatsoever,’ she said.
Ageless: Dr Haworth claims Home and Away star Ada Nicodemou, 41, has stayed ‘on point’ in her career thanks to ‘various non-surgical cosmetic treatments’. Left: in 2008. Right: in 2017
‘It is clear as day that Mr. Thorpe had a rhinoplasty,’ he said.
‘The dorsal hump of his bridge has been significantly lowered so that his tip now overprojects from his face.’
It is clear as day’: In October, it was speculated that Olympian Ian Thorpe had undergone a nose job – an assessment Dr Haworth agrees with. Pictured left: Ian in 2012, and right: in 2018
It seems that Australia’s brightest stars never seem to age.
And according to Beverly Hills-based cosmetic surgeon Dr Randal Haworth, some of these celebrities may have had a little extra help achieving their youthful looks.
From Sophie Monk‘s fillers to Ada Nicodemou’s ‘breast augmentation’ and Elle Macpherson’s ‘subtle rhinoplasty’, Dr Haworth pulls no punches when it comes to his professional assessments.
Just fillers! Dr Haworth believes Sophie Monk has not gone under the knife per se, and instead has indulged in non-surgical options such as cheek and lip fillers. Left: in 2002. Right: in 2011
Sophie Monk
Dr Haworth believes Sophie has not gone under the knife per se, but instead has indulged in some non-surgical options.
‘Lips get smaller with age not bigger but Sophie has defied that natural phenomenon, probably with the help of an injectable filler – such as Juvéderm, Restylane or even fat which is permanent,’ he said.
‘I also believe another filler such as Voluma or Restylane Lyft is responsible for her more sculpted and elevated cheekbones.’
Sophie, who hails from Queensland’s Gold Coast, has admitted to having filler to her top lip in the past, following the botched removal of a cyst.
‘Half of my lip was removed with the cyst, and I was advised to get filler in my top lip to help balance it out,’ she told Who magazine in early 2011.
As trifling as it may seem to the layperson, aesthetic surgery is serious business. Apart from obvious cosmetic ramifications, the seriousness becomes understandable when one considers that the surgeon must first make a healthy patient temporarily unwell in order to make he or she look better in the end. It is for this very reason plastic surgeons have an added unique responsibility which surgeons of other specialties simply do not bear. Choosing to undergo elective surgery is a series of decisions made by both the surgeon and the patient. As with all aspects of medicine, nothing is absolute, it is about controlling probability.
In this day and age, patients increasingly view plastic surgery as nothing more than a haircut with a short recovery, let alone one with a complication. Even under the best of hands, a complication can arise for any number of reasons and if it does, acting as a team with your surgeon is crucial. Whether following a facelift, rhinoplasty or any plastic surgery for that matter, almost all complications can be fixed in the end, even if multiple surgical revisions are needed.
It is normal for the layman to consider surgical results as either “good” or “bad”, but those adjectives can be misleading and are certainly inadequate in revealing the true story behind the result.
“Good” surgery with a complication is not the same as “bad” surgery per se. In other words, complications do not all come from “bad” surgeons and indeed, “bad” surgeons may have successfully completed an operation without encountering obvious complications. I think it fair to say most patients consider themselves as good people and if a complication happens to them, they will perceive themselves as victims of a bad surgery and by extension, a bad surgeon. So what is the difference between “bad” surgery and a “good” surgery with a complication?
Look at it this way… in any profession, there are the “good”, the “bad” and the “excellent”. For the sake of this discussion, let’s just oversimplify the comparison between “good” and the “bad”. Since plastic surgery is as much an art (or at least an artisanal craft) as it is a science, whereby results are measured both objectively and subjectively, it is not unreasonable to compare a plastic surgeon to any artist or craftsman, including sculptors, painters and woodworkers. Artists filter their talent and vision through years of experience to not only earn but continually solidify their reputation as either being “good” or “bad”. Moreover, good artists become respected by not just producing one “good” piece but doing so consistently, whereas the “bad” consistently create sub par results as judged by the median consensus.
However, all artists, whether good or bad, are limited by the quality of material with which they work. It is known that Michelangelo’s David has been deteriorating at a far more rapid pace than would be expected because of the poor quality of its marble composition. Bernini also broke a piece of marble in half through chiseling into an unexpected vein in the stone causing him to start all over with a brand-new block. Does that make him a bad artist? Hardly not.
In other words, complications happen and that’s why there are consents to protect not only the doctor but also the patient. Consents should ensure the patients are informed as to the shared risk both they and the surgeon take when undergoing surgery.
Many complications are avoidable. Both doctors and patients must do their part to optimize a certain outcome and minimize the risk of complications. Patients must avoid certain medications that may promote bleeding, cease all smoking for optimal circulation, follow instructions and take medications as prescribed. Otherwise, surgery may be self-sabotaged. On the other hand, surgeons must do their part in educating and performing the proper operation in the right patient with skill and dedication.
Other complications are unavoidable and just because they may be explainable in hindsight does not mean they were avoidable within the context they occurred. This is why it is paramount that patients disclose all of their medical history and follow their surgeon’s instructions to a T in order to minimize unexpected situations such as abnormal bleeding, poor wound healing, etc..
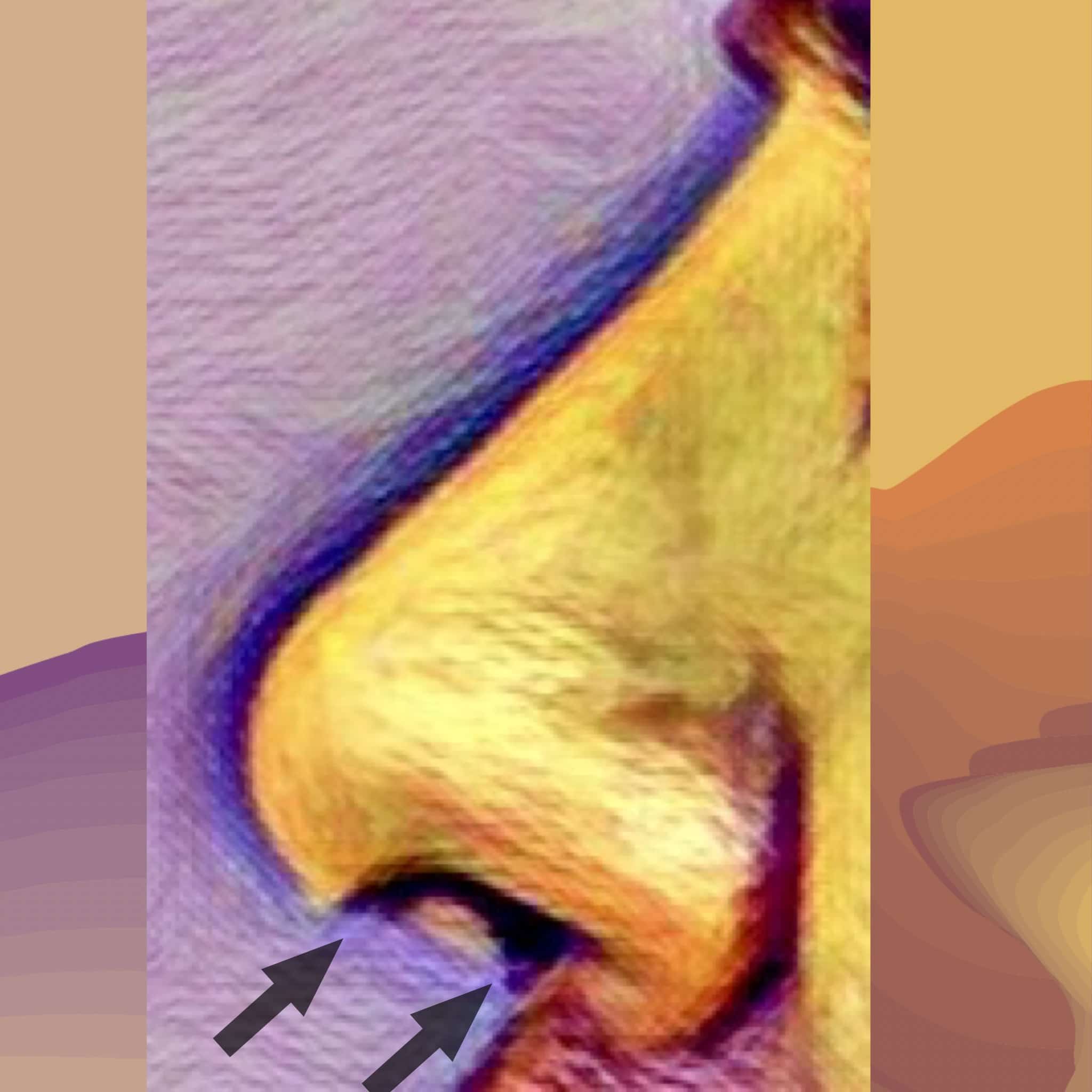
What spurred me to write this particular blog was a recent experience having performed a complex revision rhinoplasty on a dear friend of mine of 20 years. Unfortunately, this advanced detailed nasal reconstruction was exacerbated by unexpected physiological conditions including excessive bleeding and poor tissue characteristics. The next day, the patient presented with so much swelling underneath the pressure cast that it was being pushed off the face. The swelling was a hematoma which I immediately evacuated from under the skin (it was 4 1/2 mL, being the largest nasal hematoma encountered by either my colleagues or myself). Accompanying this was necrosis (death) of the columellar skin (the partition separating his left and right nostrils). This was particularly disappointing to say the least because the surgical results in terms of nasal shape, symmetry, tip definition and projection were otherwise excellent. Yet losing coverage over the columella would have serious ramifications.
Despite attempts to bring vascularized tissue using local intraoral flaps, my friend eventually needed the help of a certain specialist to bring fresh tissue to the columella below the nasal tip with a temporary forehead flap.
The arrows on the drawing illustrate that portion of the nasal skin (overlying the columella) that was necrotic. Replacement is required through vascularized tissue flaps
Albeit exceedingly rare, this 1.5 x 1.2 cm skin loss was enough to eradicate not only their trust in me as a surgeon but also our long term friendship. Most patients understandably experience a spectrum of emotions including panic, sadness, denial, anger and ultimately acceptance from a complication such as this. However, nothing could prepare me for the degree of ongoing vengeful anger and hostility the patient and their partner have directed towards me including threats to go to the press and ruin my reputation.
Anger is not only destructive but also lacks focus, therefore it can be especially counterproductive to both healing and a good result (not to mention friendship!). Premature castigations of blame fuel brash, illogical decisions which actually complicate the original complication.
Understanding the differences between “bad” and “good” surgery and “good” surgery with a complication can certainly help put things in perspective. When a patient concedes the net surgical aesthetic result, at least in terms of shape and symmetry, as good if not excellent, he or she is less likely to question, and more likely trust, their original choice of surgeon. Whether their breast lift incision opened or, as in this case, a small but strategic portion of nasal skin died, the affected patient will see the “bigger picture” and believe their surgeon will do the right thing by having their best interests at heart. This same patient understands that they were not necessarily a victim or unjustifiably punished by “bad” surgery. Instead, they will accept things for what they are, learn patience and develop a sense of optimism to set themselves up for the best possible outcome in the future.
The majority of complications concern wound healing and minor infections. For these, possible antibiotics and the “tincture of time” for healing to occur are required. Other times, simple, clinical interventions such as laser treatment, injections, the occasional scar revision and creams are all that are needed.
Other complications require more invasive solutions. Depending on the type of complication, an expeditious trip to the operatory maybe all that is required (e.g.,to drain a hematoma) whereas staged surgical revisions may be undertaken in the extremely rare case of tissue loss.
Most surgeons will recognize if a particular complication is beyond their level of expertise. A patient should not feel abandoned or simply passed off if they are referred to another expert if a complication warrants it. It is important to recognize that medicine is team work and the referral is simply a reflection of the original surgeon’s dedication to the best outcome possible.
Emotional advice after a complication
–Watch out for advice with an agenda. It is understandable that if a complication does arise, fear and anxiety will prompt you to seek solace and advice from friends and family members. While this is wholeheartedly encouraged, it is important to remember that not all the advice given is good especially considering that those giving advice are not often doctors nor do they know the intricate details of the patient’s particular case. Though most advice is well-meaning in intent, some may be motivated by guilt, jealousy, personality disorders or just plain ignorance. Furthermore, the advice a patient may obtain from elsewhere may be counterproductive because it may only increase their level of anxiety.
–Stay optimistic and avoid jumping to any pessimistic conclusions. It is not unheard of that acute anxiety will provoke a patient to impatiently reach for the help of an alternative plastic surgeon. Unfortunately, some plastic surgeons may be unscrupulous and advise the fragile, highly suggestible patient into unnecessary and ill-timed surgery claiming it is urgently needed to prevent some permanent deformity. Always keep a line of communication open with the original plastic surgeon to not only help allay personal fears but also be guided in the right direction with a second opinion if necessary.
“Time is a cruel thief to rob us of our former selves. We lose as much to life as we do to death.” Elizabeth Forsythe Hailey
Living in the modern world becomes more complex and harder as life in the 21st-century becomes faster and faster. We are burdened with responsibilities and distracted by an interminable onslaught of media in all forms including the capricious internet. It seems as if everything is competing for our attention in one way, shape or form while stealing precious time we could otherwise devote to family, friends and simply to our own selves. Therefore, when it comes to saving time, the need to heal quickly after any cosmetic procedure is almost rapacious.
Unfortunately, there is no magic pill or formula to bypass the post operative inflammation of bruising, swelling and discomfort at this current time. As one of the top plastic surgeons in Beverly Hills, Dr. HAWORTH has seen a thing or two about how patients heal after the thousands of surgeries he has performed over two decades. As a facial plastic surgery expert, he has performed thousands of primary and revision rhinoplasties, brow lift, facelifts and blepharoplasties not to mention the breast implant operations throughout his career and has realized there are things you can do both at home and in the clinical setting to accelerate your healing.
First of all, it is a good idea to focus on whole foods as much as possible while avoiding processed ones as the former will contain the highest levels of vitamins and amino acids your body will need for a speedy recovery. Amino acids help wounds heal faster and obviously, these are found in chicken, meats, egg whites, fish, brown rice, healthy nuts like walnuts and almonds or sunflower seeds. Taking supplemental vitamin C in your diet while increasing zinc in your diet can be helpful. Instead of taking vitamin C for a bottle, you can eat strawberries, papayas and citrus fruits which are great sources of vitamin C. 500-1000mg is the usual amount that is taken. Zinc is found in oysters which have one of the highest levels of zinc found in any food. If you are going to take a supplement, 15 mg of zinc daily is the recommended amount but you can increase your zinc intake to 30–50 mg for 2 weeks before and 2 weeks after surgery, using zinc picolinate.
Beverly Hills plastic surgeon Dr. Haworth also recommends these useful supplements to take in preparation for your surgery include:
B12 and Iron – Iron and B12 both aid bone marrow in forming new blood cells, so incorporate foods like fish and eggs.
Vitamin B6250mg, twice a day for a week, starting 3 days after surgery. This helps reduce post-surgical fluid retention, such as swelling of the face, hands, feet or legs. With B6, you can experience substantial reduction within 24 to 48 hours.
CoQ10- Surgical trauma (particularly from cardiac surgery) causes an increase in free radicals, which damage cellular function. For this reason alone, you should take at least 50 mg of CoQ10 as part of your daily routine before your cosmetic surgery and 100–200 mg/day for at least 4 weeks after.
Fiber and probiotics – This combination helps boost the immune system and also keeps your digestive tract moving along. Eating yogurt with granola is just one easy way to get a serving of both fiber and probiotics! When choosing a probiotic, consider one that contains acidophilus and bifida bacteria (follow label instructions for dosage). Surgical patients often receive oral or intravenous antibiotics in the hospital, which creates the potential for yeast infections, digestive disturbances and diarrhea. A probiotic may help counteract these problems.
One amino acid that has been shown to speed with healing is glutamine and a study from Harvard and Dave showed that it shortened healing by about four days. Apart from supplements, glutamine can be found in beef, chicken and all types of fish. Dairy products such as cheese, milk, yogurt and eggs contain glutamine with ricotta and cottage cheese being the two richest sources. Vegetarians can find glutamine in beans and lentils.
For most of his patients, facial plastic surgery specialist Haworth recommends supplemental Arnica Montana, Bromelain/ Bromezyme (this pineapple enzyme helps prevent blood clots, aids digestion while decreasing inflammation and pain after surgery) and Pycnogenol/Pine bark. This triumvirate is aimed at reducing bruising, soreness and inflammatory edema.
Apart from the above, many patients inquire about any other additional medications, exercises or procedures that can be done to maximally reduce their healing times after surgery. Of course, all patients should ask their individual physicians or surgeons about their own personalized recommendations to speed up recovery which is beyond the scope of this post.
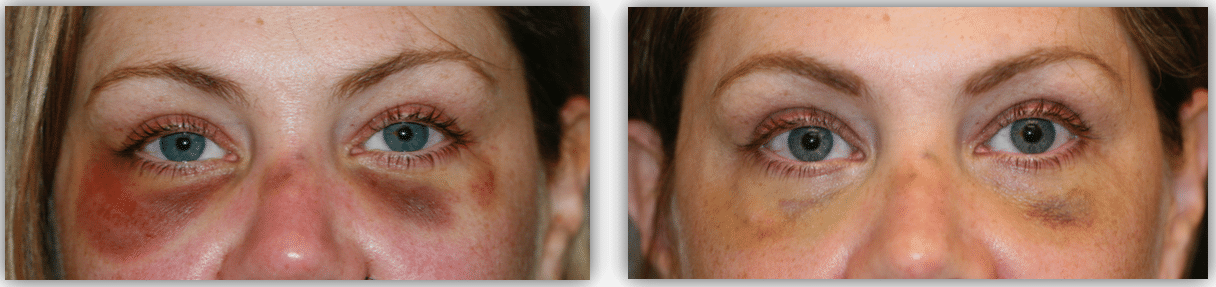
Bioptron® Light employs a combination of polarized infrared and visible light (480nm-3400nm) considered beneficial in the treatment of wound problems and injuries by exerting its effect at the cellular level. Bioptron® therapy has a low energy density (fluency) of 2.4 J/cm2 at a distance of 10 cm and can penetrate the skin up to 2.5 cm.
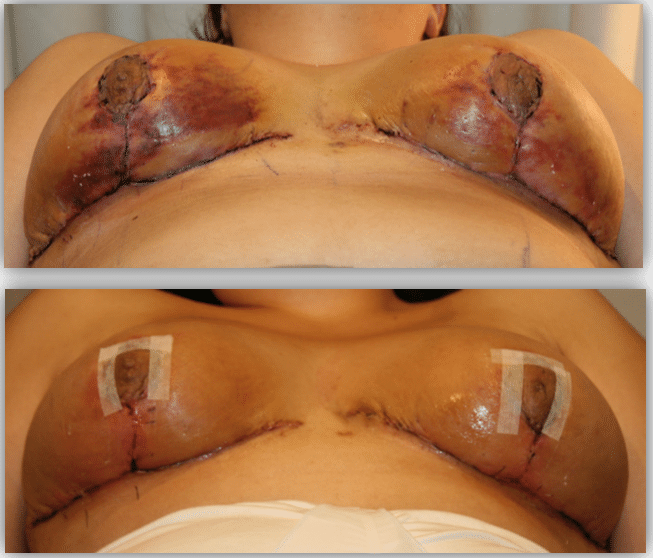
This patient had impending skin necrosis around her here after a facelift. Only 7 days of Bioptron ® light therapy were administered and notice the rapid improvement in reversing the damage.After 5 days of Bioptron® therapy to resolve bruising resulting from lower eyelid procedure to treat her dark circles/tear troughs.After 3 days of Bioptron® light therapy to accelerate the resolution of bruising and skin injury after a breast reduction by Dr. HAWORTH.
It has been used effectively in the treatment of burns, pressure sores, leg ulcers, wounds, pain and recently, postoperative healing. Dr Haworth have found it very useful in his clinic to reduce both swelling and bruising. Supporting his experience, other plastic surgeons here and abroad have noted decreased resolution times of eccymosis and edema following surgery by over 33% with Bioptron®. Indeed, it has been used to also reverse the course of cutaneous necrosis as well as accelerate granulation of open wounds, either alone or in conjunction with hyperbaric oxygen therapy (HBOT).
Hyperbaric oxygen therapy involves breathing pure oxygen in a pressurized room or tube. It is a well-established treatment for decompression sickness, a hazard of scuba diving. Other conditions treated with HBOT include serious infections, bubbles of air in blood vessels and non-healing wounds as a result of diabetes or radiation injury.
In a HBOT chamber, the air pressure is increased to 3 times higher than normal air pressure and under these conditions, your lungs can gather more oxygen than would be possible breathing pure oxygen at normal air pressure. However, there is some confusion about what actually is “true” HBOT. Those employing “soft” tent like enclosures are essentially useless since they are unable to obtain a true hyperbaric environment of 2 to 4 atmospheres absolute (ATA). In fact, these personal or home-use “hyperbaric” tent enclosures can usually only attain a pressure of 1.3 ATA. There is a debate as to how much and how many treatments are necessary to speed up recovery after plastic surgery. While most plastic surgeons perhaps recommend one preoperatively and at least 3 to 5 postoperatively, experts in the field say one needs at least 15 to 20 treatments in order to see significant results. In my experience, 3 to 5 treatments are all that is necessary to achieve the more modest goals of reducing edema, bruising and discomfort resulting from elective plastic surgery.
After certain surgeries, body contouring plastic surgery expert Dr Randal Haworth may also recommend selective lymphatic massage/drainage to resolve edema (swelling) of the extremities, particularly after liposuction or liposculpture.
The above aforementioned vitamins, nutritional supplements and clinical interventions may not be the panacea to surgical healing which comes in a pill form, but they certainly are a step in the right direction in making recovery from any procedure as smooth as possible in 2017.
While we in the cosmetic industry are getting better and better at delivering the results that patients expect, I still hold fast that 60 to 70% of modern high-tech materials and devices in plastic surgery over promise and under deliver !
Considering that the future of plastic surgery will be less about actual surgery as more more and more technological advances are made in the lab (think genetic engineering, better fillers, better lasers, etc.), this 60-70% statistic is rather disappointing. What makes this all the more egregious is the fact that doctors are forced to pay an arm and a leg for such underperforming technologies (Ulthera ® Thermage®, etc.). In light of the fact you can get a state-of-the-art Tesla with all the bells and whistles for around $100,000, paying $150,000 or more for a machine that just delivers fuddy-duddy ultrasound technology through a wand to aid in liposuction is frankly outrageous. However, the medical tech companies can’t be solely blamed for this-they are basically governed by the FDA’s policies which, in turn, are a response to precedents extrapolated to an absurd degree by lawyers.
Unfortunately, I have seen it all too many times – a new plastic surgery technology coming out amidst a flurry of media only to fade into relatively rapid obscurity. This is similar to a Billboard chart topper only to turn out to be a one-hit wonder!
In my opinion the latest overhyped snakeoil is Kybella® from the big pharma conglomerate Allergan®, proud makers of Latisse®, Botox®, Voluma®, Juvéderm®, etc.
I was glad to hear from some of my esteemed colleagues at the recent American Society of Plastic Surgery meeting in Los Angeles that their thoughts on Kybella ® echoed mine.
Taking into account Kybella’s negative points, which include:
1. relative risk of damaging important facial nerves,
2. cost (though one treatment is less expensive than liposuction, more often than not multiple treatments are necessary and these, of course, add up),
3. associated pain,
4. longer recovery (which, ironically, is worse than surgical liposuction since remarkable swelling can occur after every injection session)
and
5. inferior results to those obtained with aesthetically and skillfully performed liposuction
…there is little to no advantage in utilizing Kybella® for my patients except perhaps for its superior multi-million dollar marketing campaign! Indeed, micro liposuction can provide unprecedented control in removing fat to treat a double chin while refining the jawline and addressing the jowls as well-all with less downtime and more economically so in the end.
Case in point:
Dramatic perioral rejuvenation including improvement of the jowl and chin utilizing a combination micro liposculpture and fat transferDramatic perioral rejuvenation including improvement of the jowl and chin utilizing a combination micro liposculpture and fat transfer. Note the smoother jawline and submental (chin) region all performed with delicate no scar facial surgery without a face or neck lift.After combination micro liposculpture and fat transfer. Note the smoother jawline and submental (chin) region all performed with delicate no scar facial surgery without a face or neck lift.